Yale is a famous institution with a renowned hospital known for the discovery of innovative medical practices that have saved lives and bettered humanity. However, Yale also has a dark history. From the Skull and Bones secret society of elites, to its founder being a racist slave trader. Yale University, named after Elihu Yale, the President of the East India Company in St George, India, was a slave owner and trader. A famous painting that hangs on the campus of Yale depicts him with a young boy with a chain around his neck.
It feels like there are chains of COVID around our necks now with mandated vaccination, masking, testing, restrictions and lockdowns, now being a requirement, or threatened, in order to work and live in society. If we lose control over our own bodies, we will become slaves for a perception of safety. There is no other freedom more important than bodily autonomy and informed consent. Yale New Haven is the primary teaching hospital for the Yale School of Medicine. Yale sets the precedent for common accepted medical practices.


We are told we are not smart enough to read the science, we are told to trust the experts. What happens when the experts are wrong? Why shouldn’t we read the science and make an informed decision? How have we gotten to this place in society where segregation has made a comeback in the guise of public health? Yet this narrative, “It’s for your own good, and the good of others,” has always been the slippery slope to tyranny. History is full of these stories. The Nazis used typhus, lice, and tuberculosis, to put Jewish people, gypsies, and anyone else they did not care for into concentration camps for the safety of the public. Australia is building “quarantine camps” as I type, for the safety of the public. Last year New York State introduced Assembly Bill A416, a quarantine law that could lock people up and treat them medically whether the quarantined wanted it or not, for the safety of the public. This bill still sits in committee:
“UPON DETERMINING BY CLEAR AND CONVINCING EVIDENCE THAT THE HEALTH OF OTHERS IS OR MAY BE ENDANGERED BY A CASE, CONTACT OR CARRIER, OR SUSPECTED CASE, CONTACT OR CARRIER OF A CONTAGIOUS DISEASE THAT, IN THE OPINION OF THE GOVERNOR, AFTER CONSULTATION WITH THE COMMISSIONER, MAY POSE AN IMMINENT AND SIGNIFICANT THREAT TO THE PUBLIC HEALTH RESULTING IN SEVERE MORBIDITY OR HIGH MORTALITY, THE GOVERNOR OR HIS OR HER DELE- GEE, INCLUDING, BUT NOT LIMITED TO THE COMMISSIONER OR THE HEADS OF LOCAL HEALTH DEPARTMENTS, MAY ORDER THE REMOVAL AND/OR DETENTION OF SUCH A PERSON OR OF A GROUP OF SUCH PERSONS BY ISSUING A SINGLE ORDER, IDEN- TIFYING SUCH PERSONS EITHER BY NAME OR BY A REASONABLY SPECIFIC DESCRIPTION OF THE INDIVIDUALS OR GROUP BEING DETAINED. SUCH PERSON OR GROUP OF PERSONS SHALL BE DETAINED IN A MEDICAL FACILITY OR OTHER APPRO- PRIATE FACILITY OR PREMISES DESIGNATED BY THE GOVERNOR OR HIS OR HER DELEGEE AND COMPLYING WITH SUBDIVISION FIVE OF THIS SECTION.”
Assembly Bill 416
We are in very dark times where nothing quite makes sense, and the people who are supposed to know what to do i.e. the experts, flip and flop, or they are just outright wrong! Whatever the motive or narrative may be, it is time to set the record straight and call them out on this. We have common law for a reason. Our Constitution endows us with bodily autonomy, the right of privacy, and the right to be secure in our persons. Viruses have plagued humanity since the beginning of time, viruses will never go away. No government, nor expert, can eradicate viruses. A virus is going to virus and run its course. We have to learn to live with it.
Will we allow ourselves to repeat a brutal human history where we are segregated, locked in camps, and treated medically against our will? We are at a pivotal time. This brave insider at Yale New Haven has given us peak at the medical hierarchy that decides what medical information, treatment, and studies, are accepted. What they reveal is quite shocking.
Package Insert – COMIRNATY
8.2 Lactation
Risk Summary
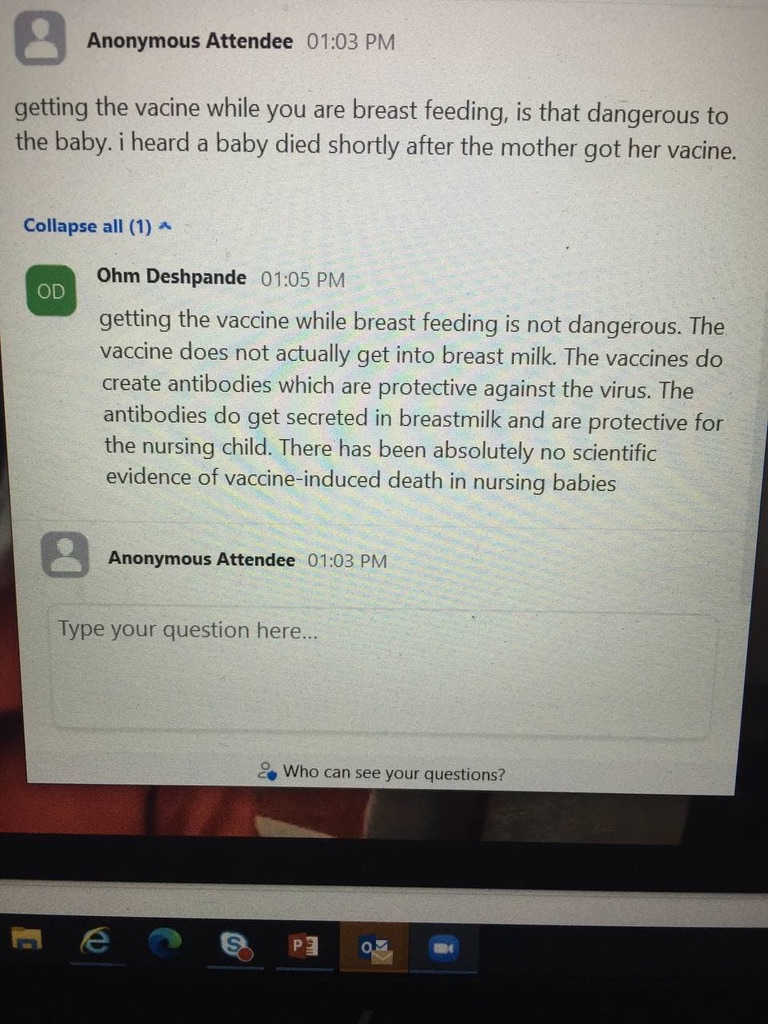
It is not known whether COMIRNATY is excreted in human milk. Data are not available to assess the effects of COMIRNATY on the breastfed infant or on milk production/excretion. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for COMIRNATY and any potential adverse effects on the breastfed child from COMIRNATY or from the underlying maternal condition. For preventive vaccines, the underlying maternal condition is susceptibility to disease prevented by the vaccine.
8.4 Pediatric Use
Safety and effectiveness of COMIRNATY in individuals 16 through 17 years of age is based on safety and effectiveness data in this age group and in adults [see Adverse Reactions (6) and Clinical Studies (14.1)].
The safety and effectiveness of COMIRNATY in individuals younger than 16 years of age have not been established.
The Vaccine Adverse Events Reporting System aka VAERS was established by the Federal Government after the 1986 Vaccine Injury Act was signed into law by Ronald Reagan. The Vaccine Injury Act gave indemnity to all vaccines on the Childhood Vaccine Schedule recommended by the CDC, and sometimes required for entry into school. Adults also take vaccines on the Childhood Vaccine Schedule. The vaccine law also required that all injuries from vaccination be reported. To compensate for vaccine injury, the government established a vaccine court. People injured by a vaccine, were mostly children, could seek compensation for an injury from the Vaccine Court.
VAERS was established to track vaccine injuries since liability was removed, this system would alert the government of a problem. Since the passage of the Vaccine Injury Act, the Federal Government has paid out over 4 billion dollars to the vaccine injured. Interestingly, VAERS, which has been around since 1990, is a passive reporting system that many people do not even know about, and that includes doctors. A study was commissioned by the government with a million dollar grant to Harvard to find out how the system was working. The results are disturbing.
According to the Harvard Study:
Electronic Support for Public Health–Vaccine Adverse Event Reporting System (ESP:VAERS)
“Adverse events from drugs and vaccines are common, but underreported. Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported. Low reporting rates preclude or slow the identification of “problem” drugs and vaccines that endanger public health. New surveillance methods for drug and vaccine adverse effects are needed. Barriers to reporting include a lack of clinician awareness, uncertainty about when and what to report, as well as the burdens of reporting: reporting is not part of clinicians’ usual workflow, takes time, and is duplicative. Proactive, spontaneous, automated adverse event reporting imbedded within EHRs and other information systems has the potential to speed the identification of problems with new drugs and more careful quantification of the risks of older drugs.”
“Unfortunately, there was never an opportunity to perform system performance assessments because the necessary CDC contacts were no longer available and the CDC consultants responsible for receiving data were no longer responsive to our multiple requests to proceed with testing and evaluation.“
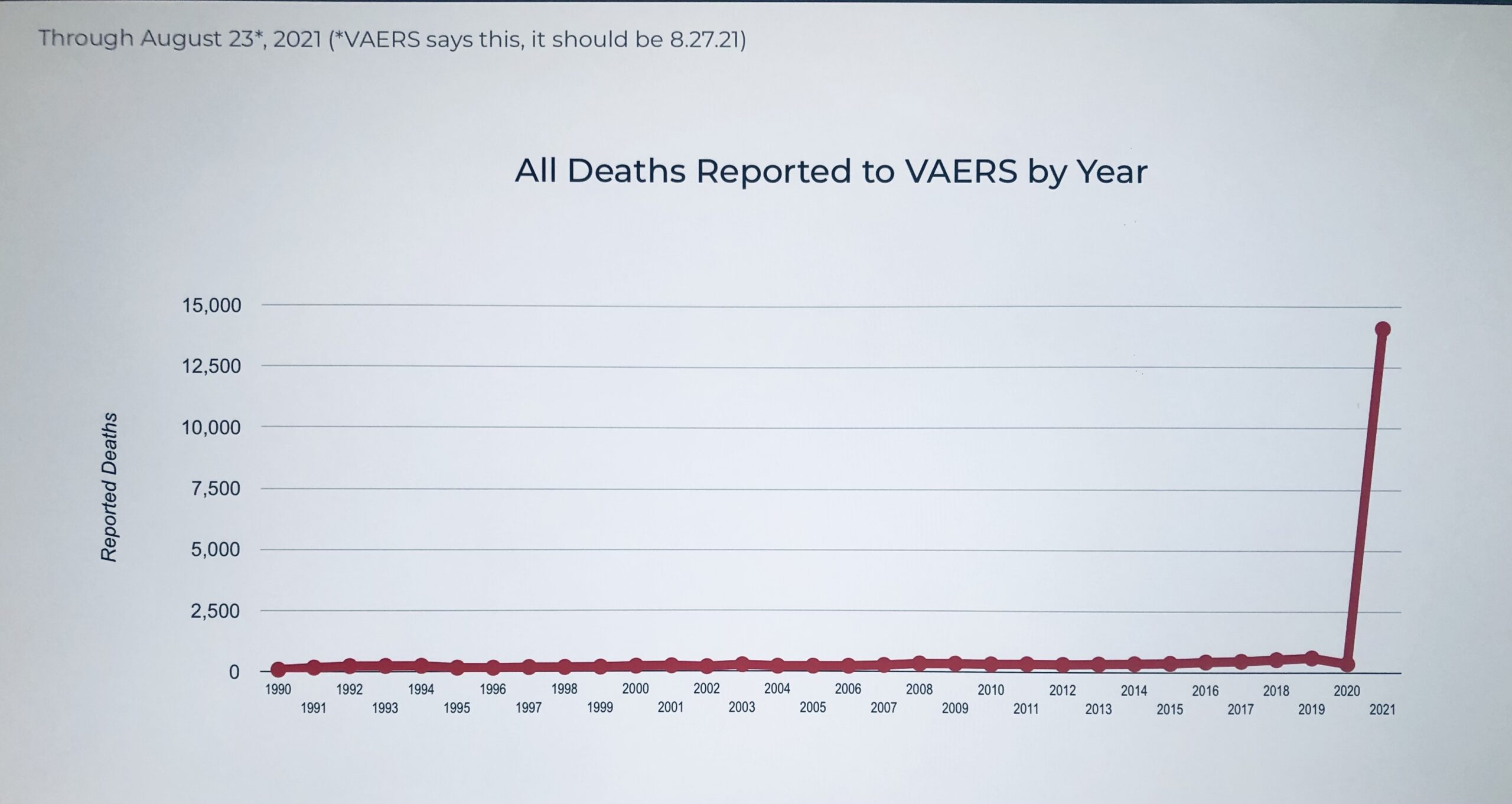
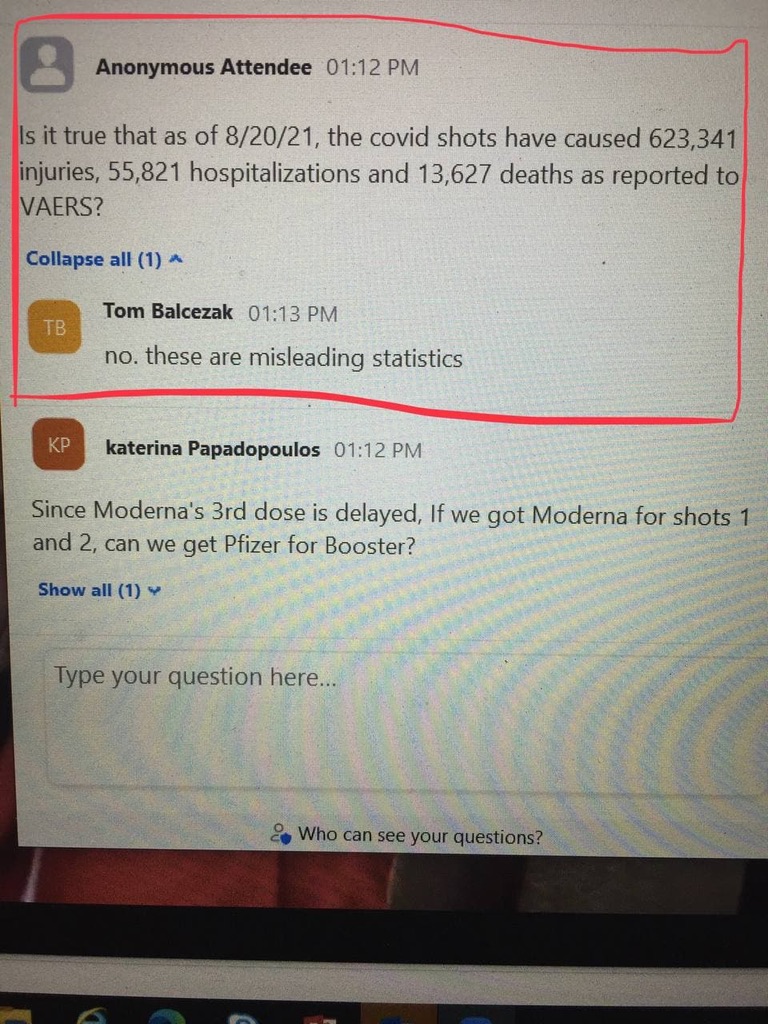
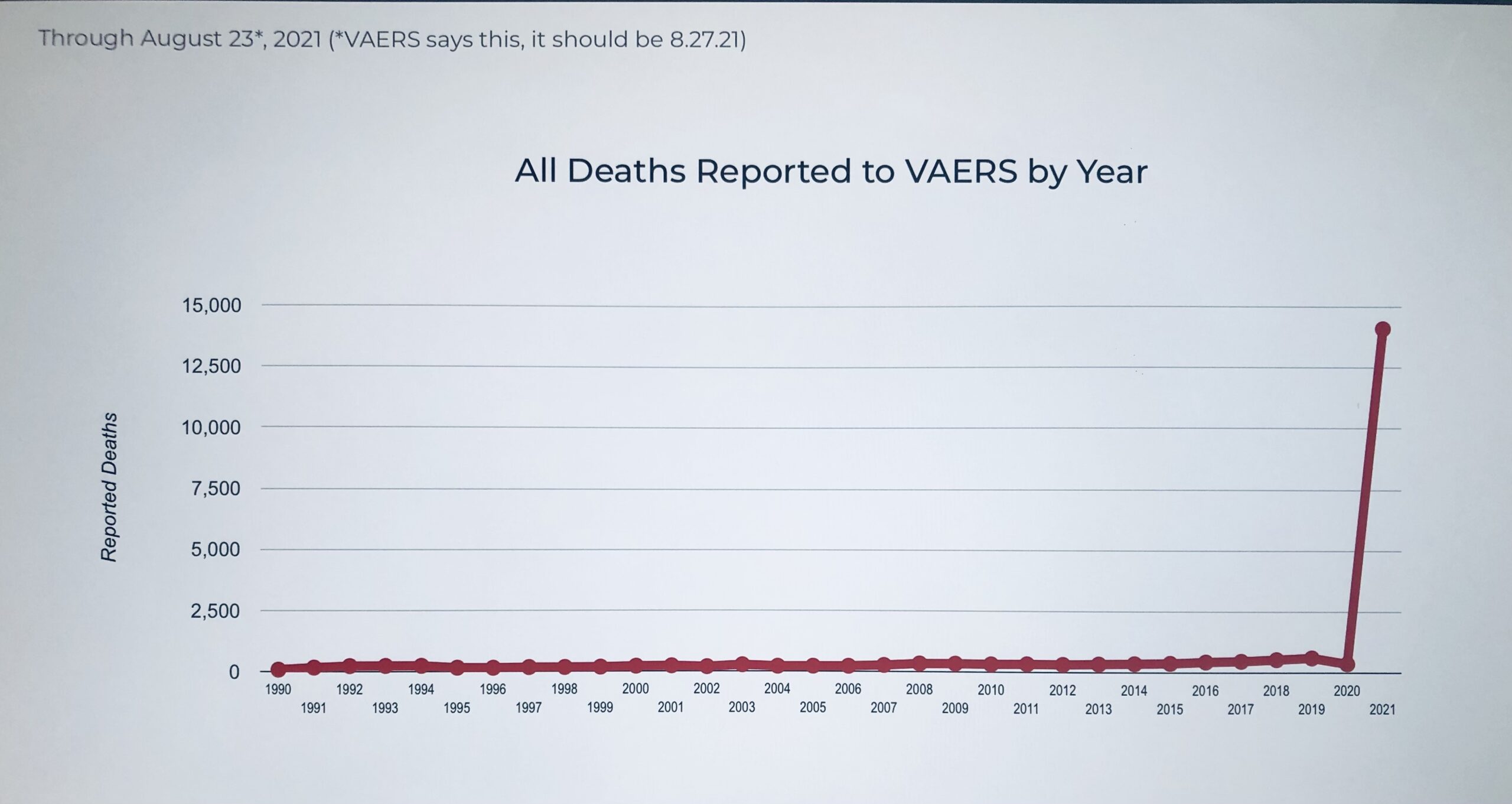
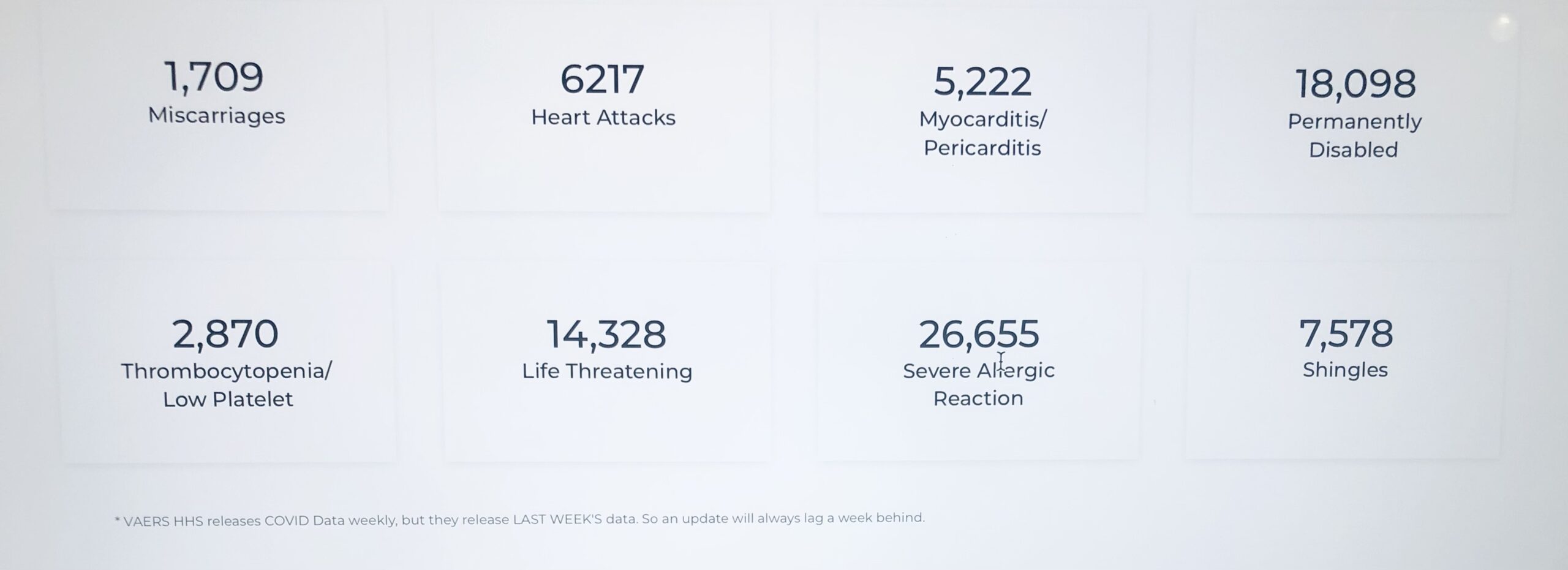
VAERS reports show an alarming spike in deaths in 2020. How can Yale New Haven just ignore this? You can read the data for yourself, and I suggest that you do. All resources are linked at end of post.
From OpenVAERS.com:

Yale Doctor on Vaccine Efficacy
According to a PubMed.gov study on informed consent,
” Results of the study: COVID-19 vaccines designed to elicit neutralising antibodies may sensitise vaccine recipients to more severe disease than if they were not vaccinated. Vaccines for SARS, MERS and RSV have never been approved, and the data generated in the development and testing of these vaccines suggest a serious mechanistic concern: that vaccines designed empirically using the traditional approach (consisting of the unmodified or minimally modified coronavirus viral spike to elicit neutralising antibodies), be they composed of protein, viral vector, DNA or RNA and irrespective of delivery method, may worsen COVID-19 disease via antibody-dependent enhancement (ADE). This risk is sufficiently obscured in clinical trial protocols and consent forms for ongoing COVID-19 vaccine trials that adequate patient comprehension of this risk is unlikely to occur, obviating truly informed consent by subjects in these trials.
Conclusions drawn from the study and clinical implications: The specific and significant COVID-19 risk of ADE should have been and should be prominently and independently disclosed to research subjects currently in vaccine trials, as well as those being recruited for the trials and future patients after vaccine approval, in order to meet the medical ethics standard of patient comprehension for informed consent.”

Hospital Dashboard 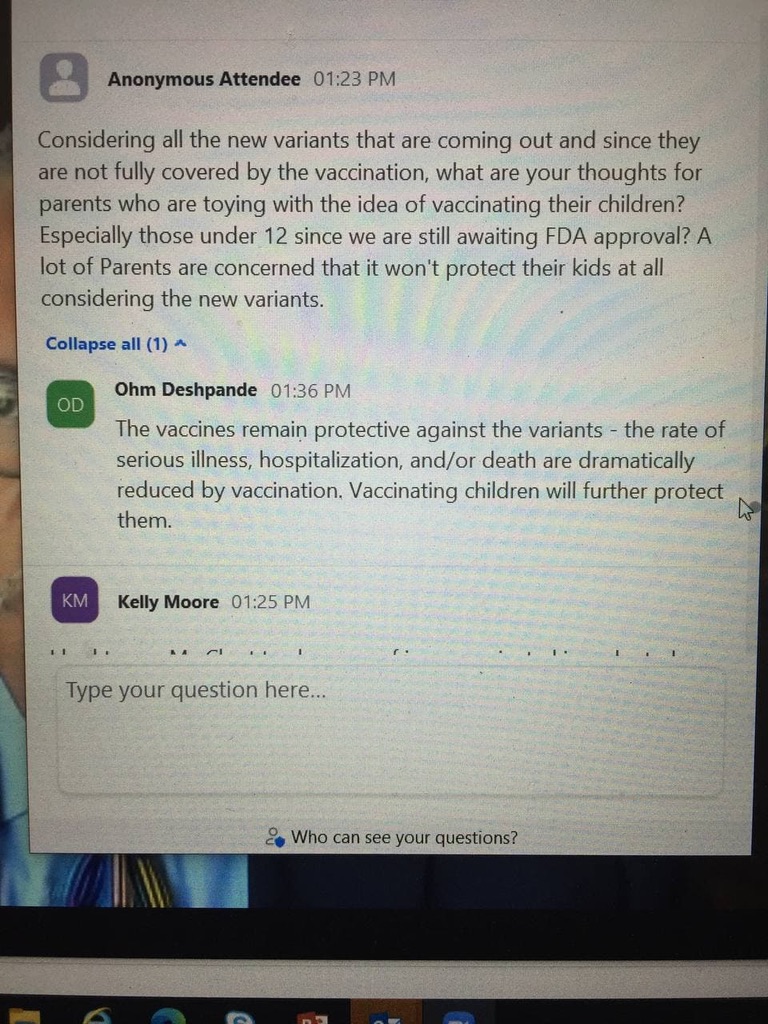
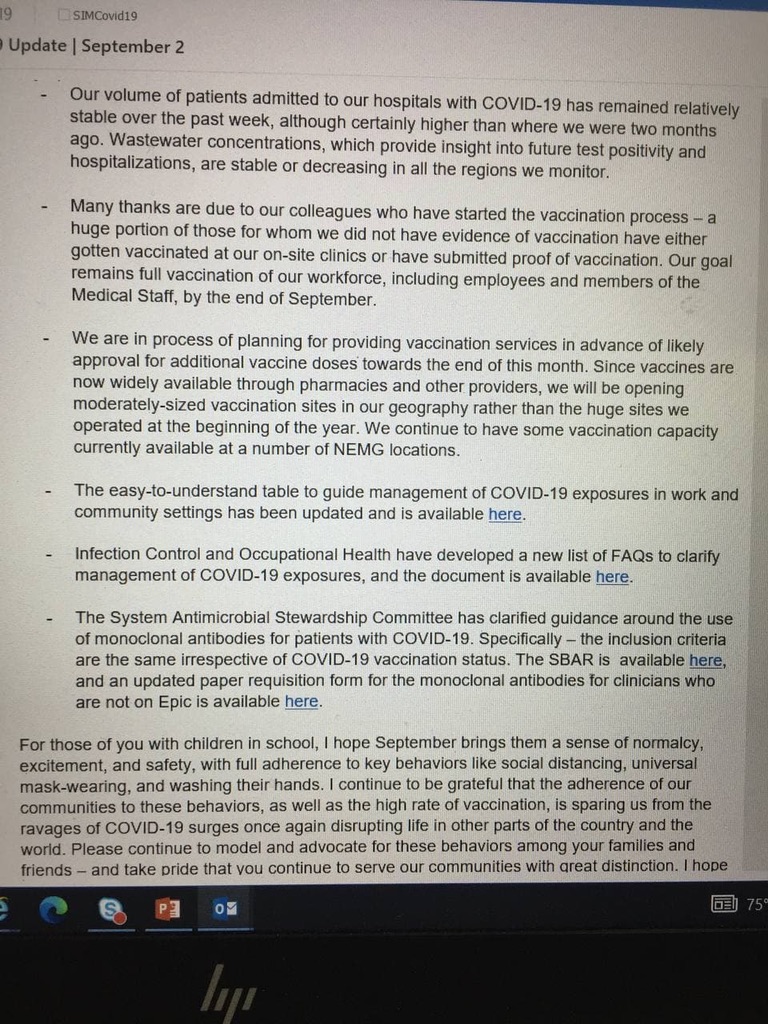
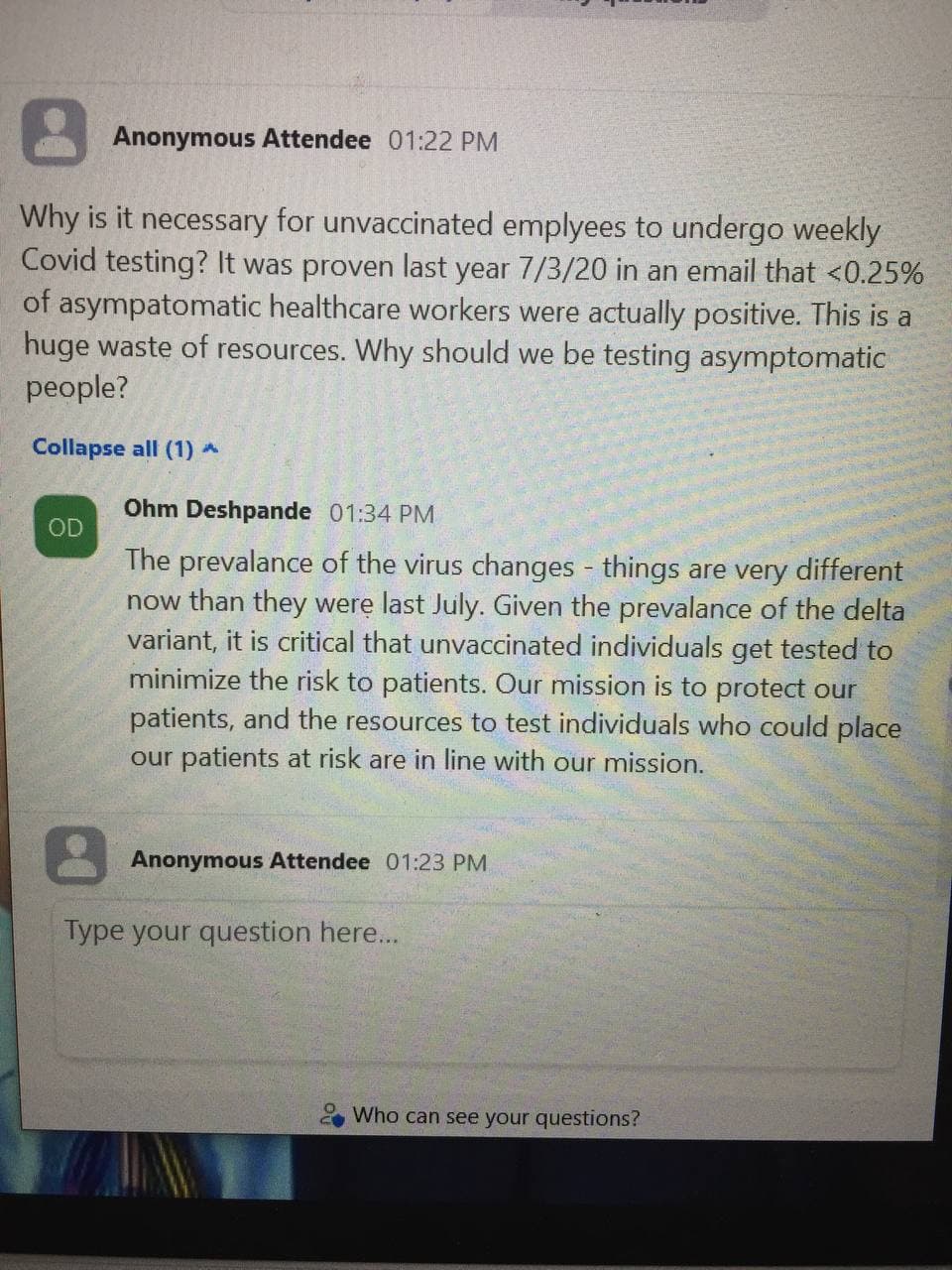
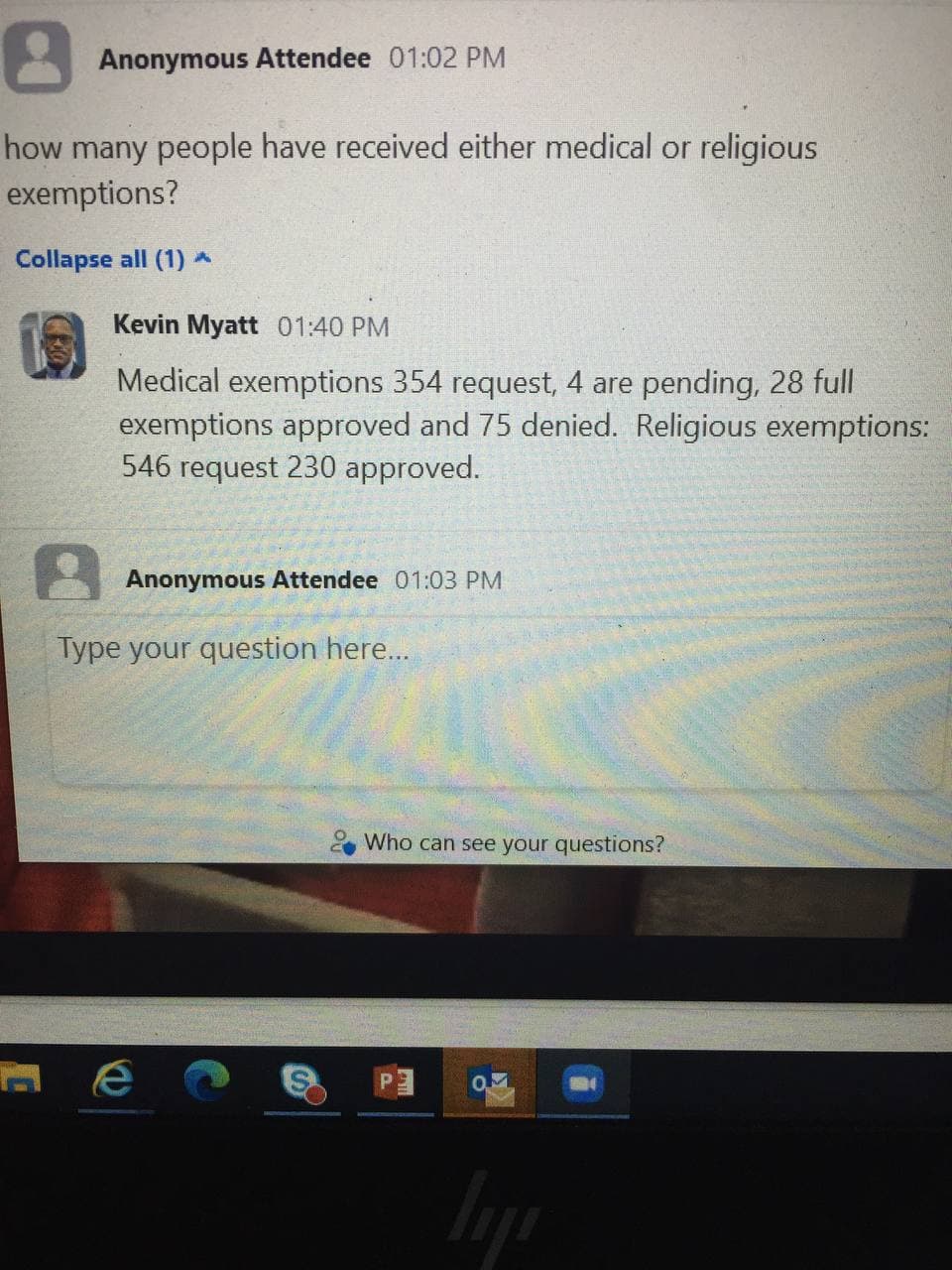
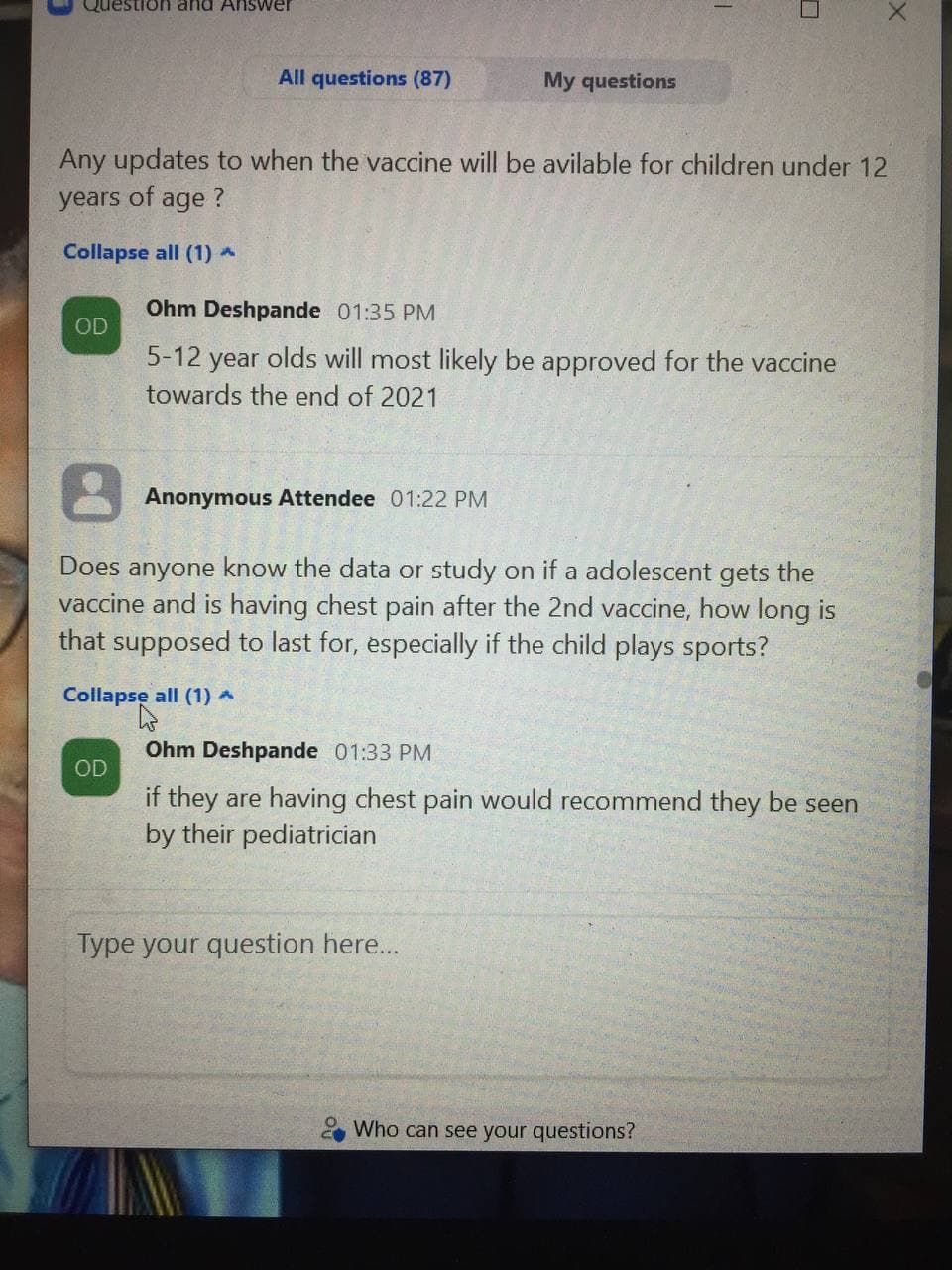
Internal Memo
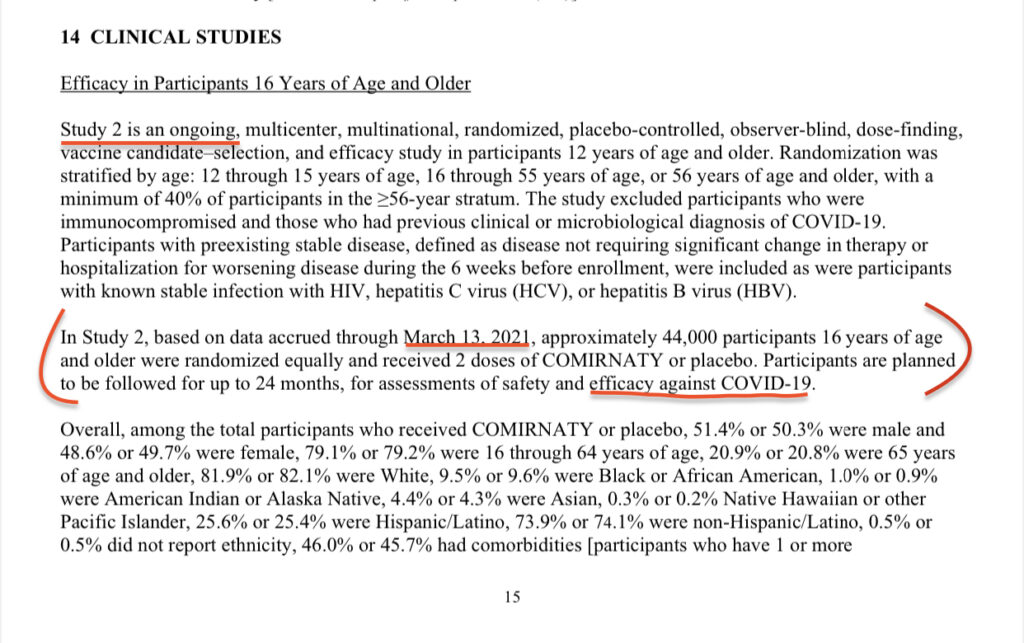
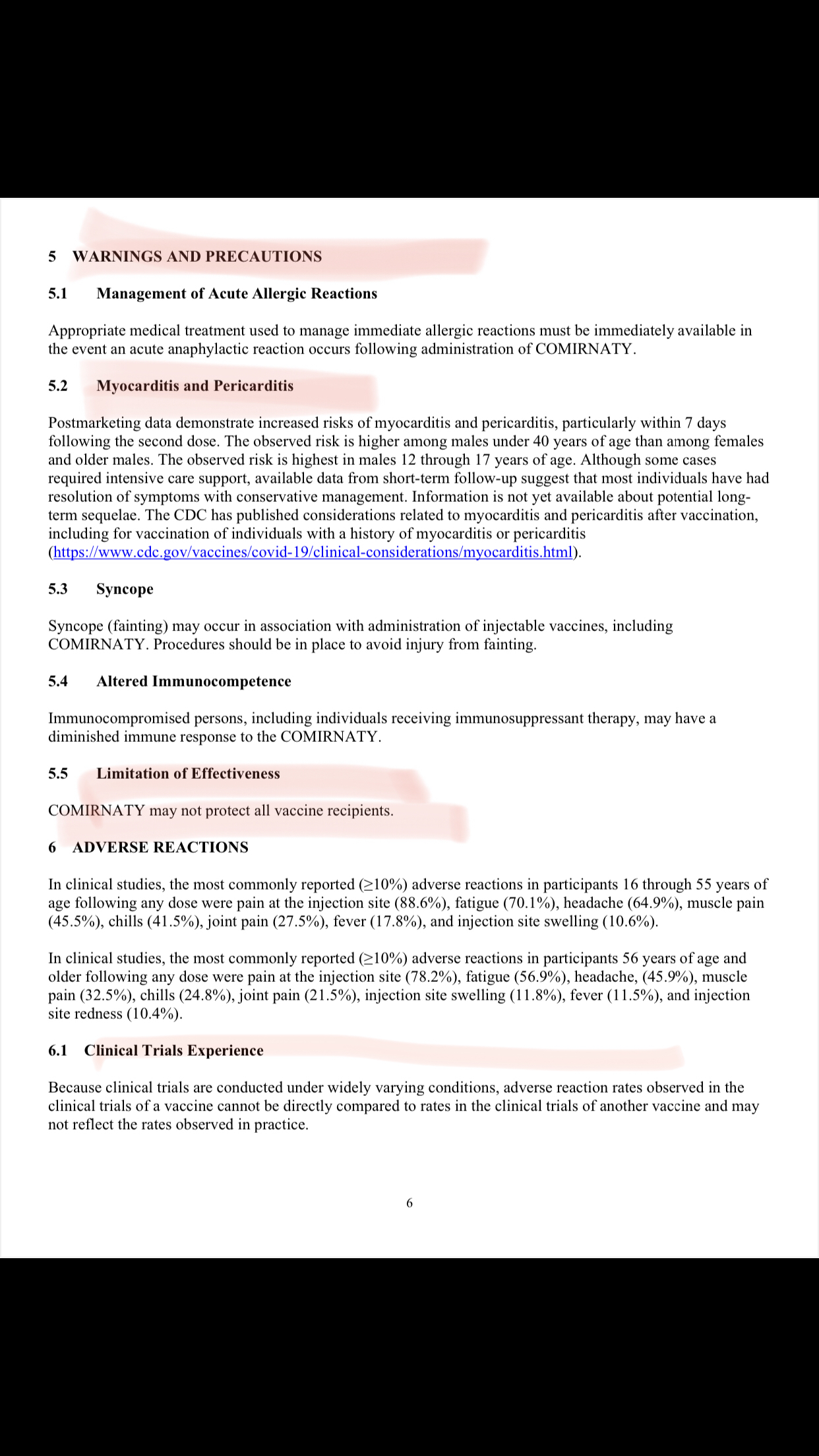
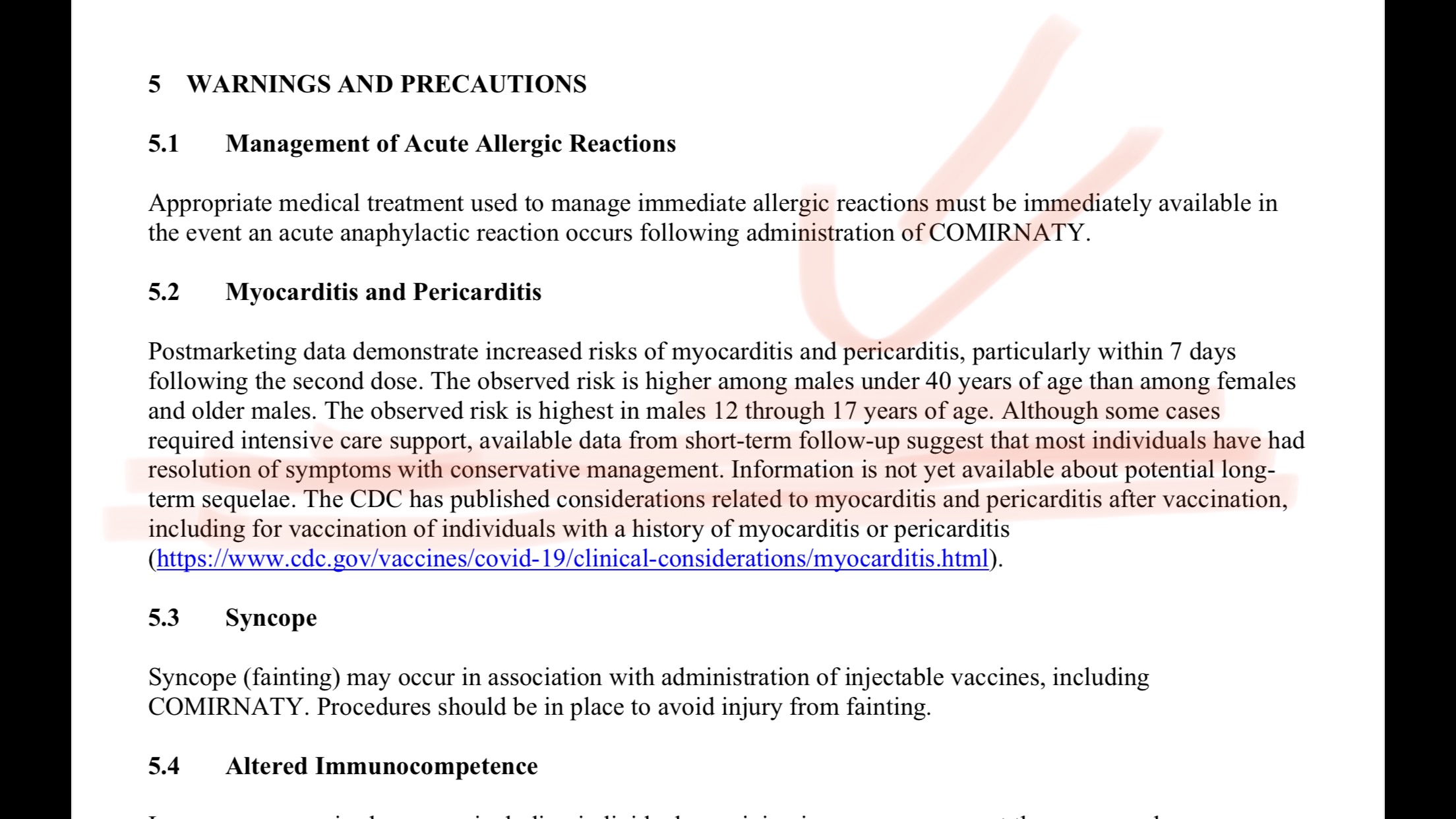
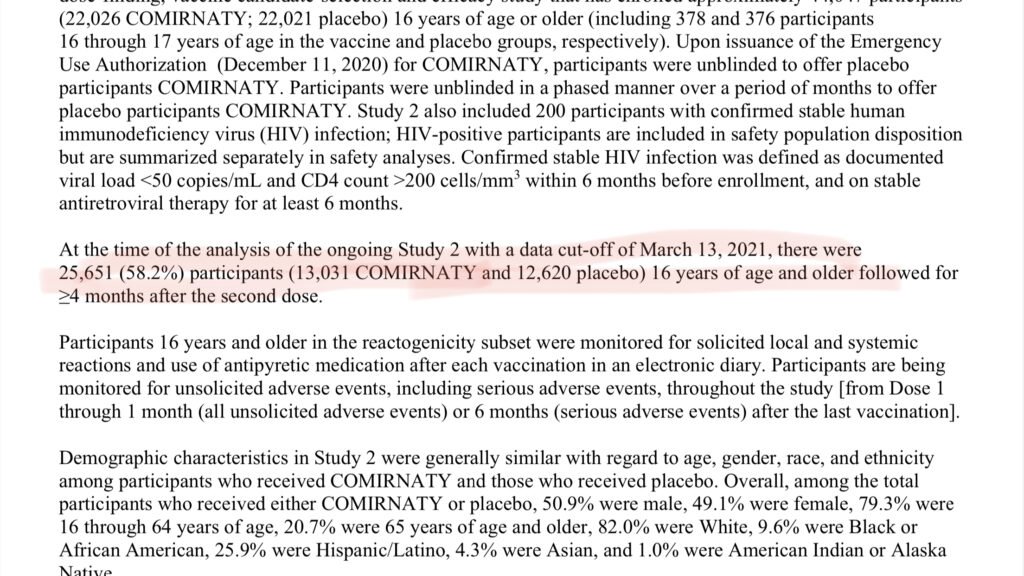
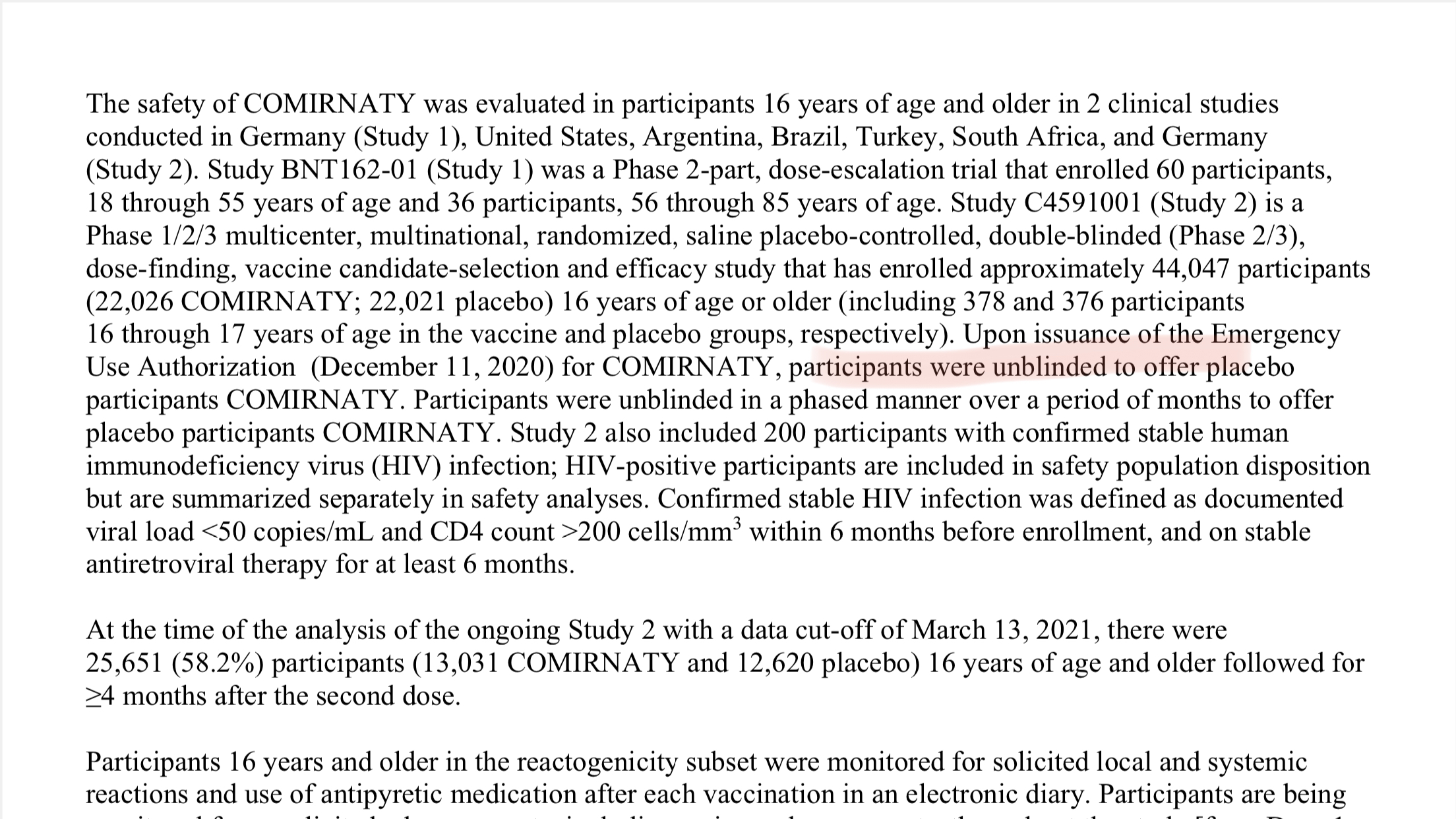
Vaccine Package Insert for the recently approved Pfizer vaccine now known as Comiranty

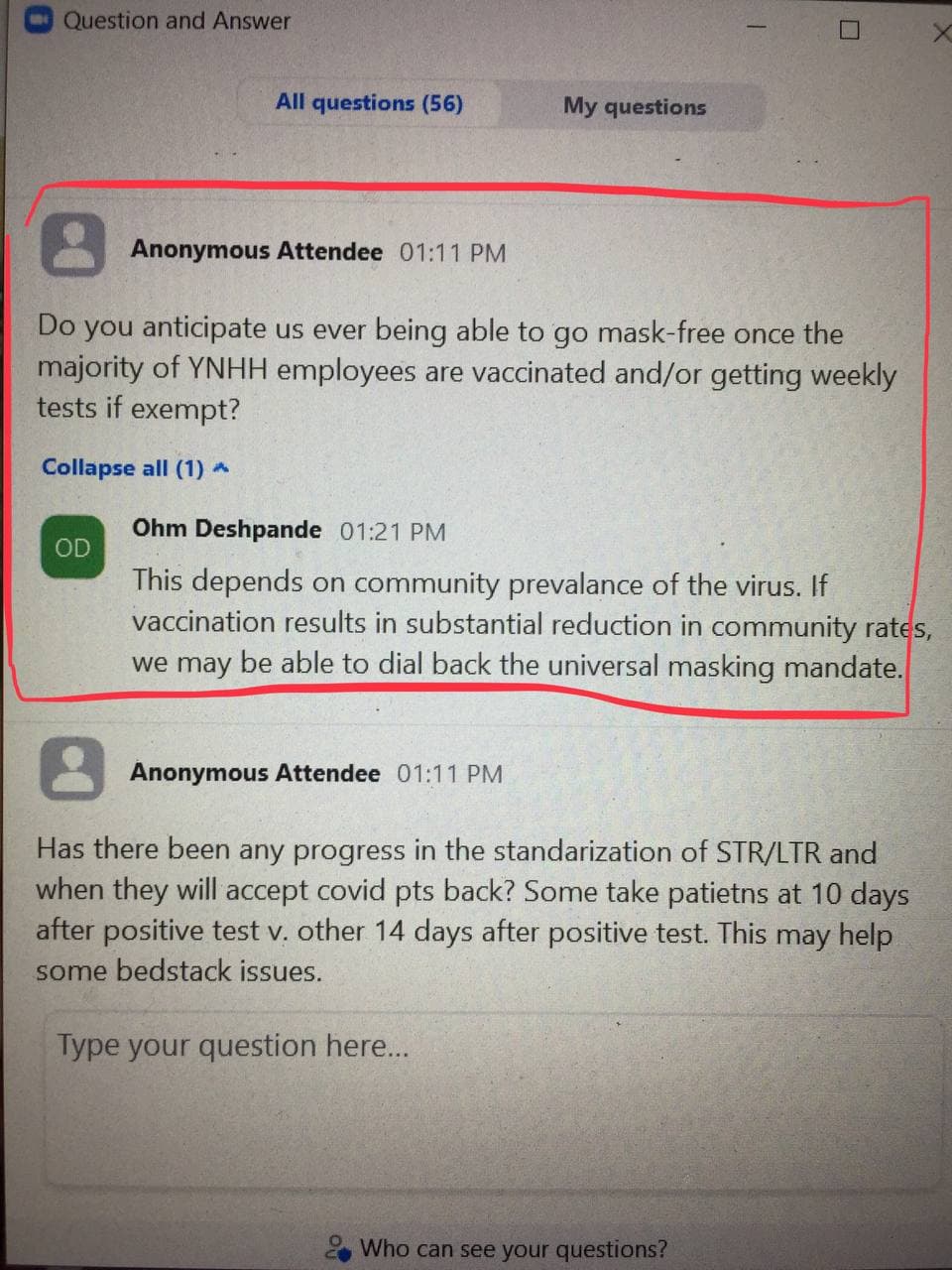
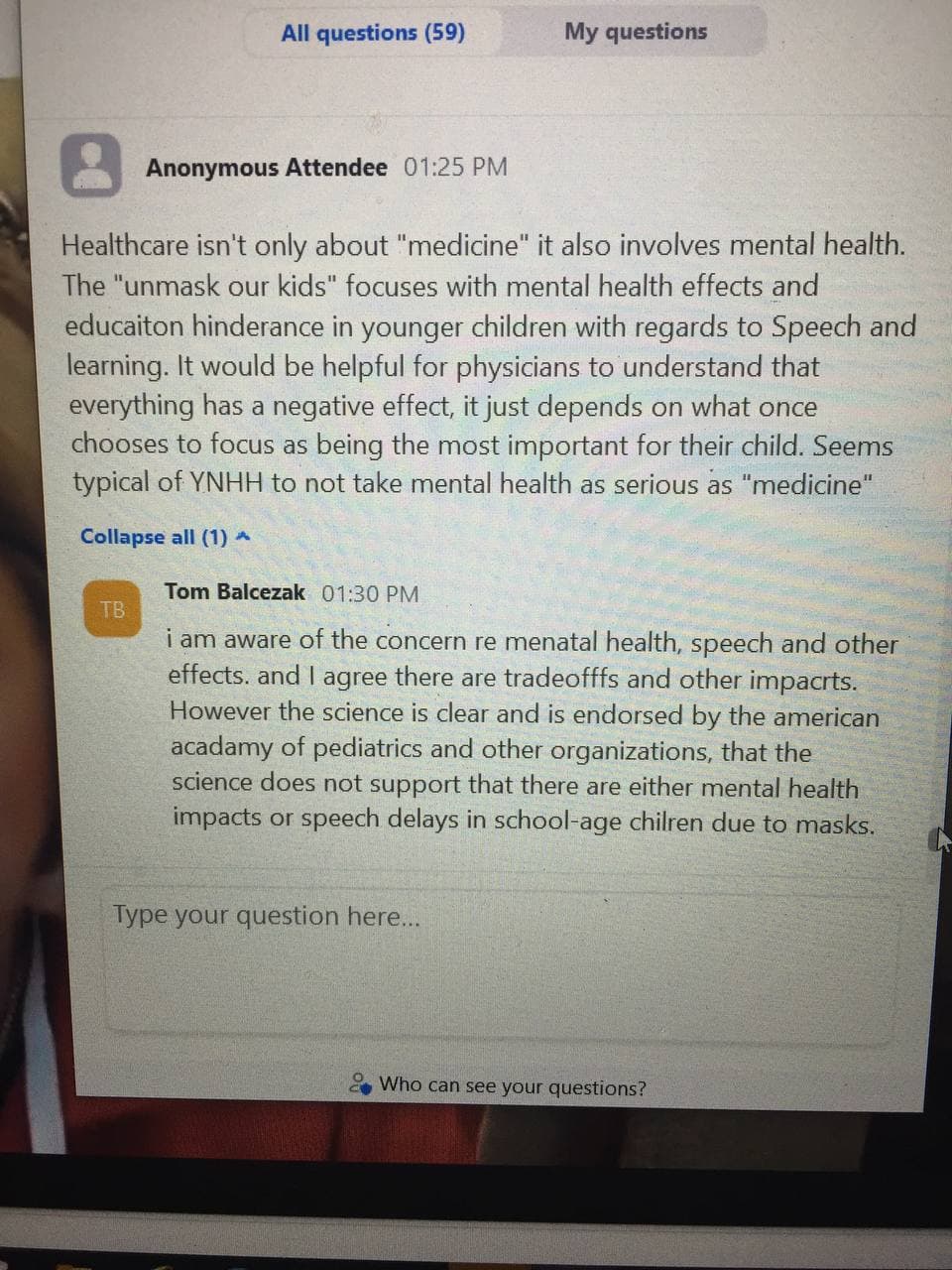
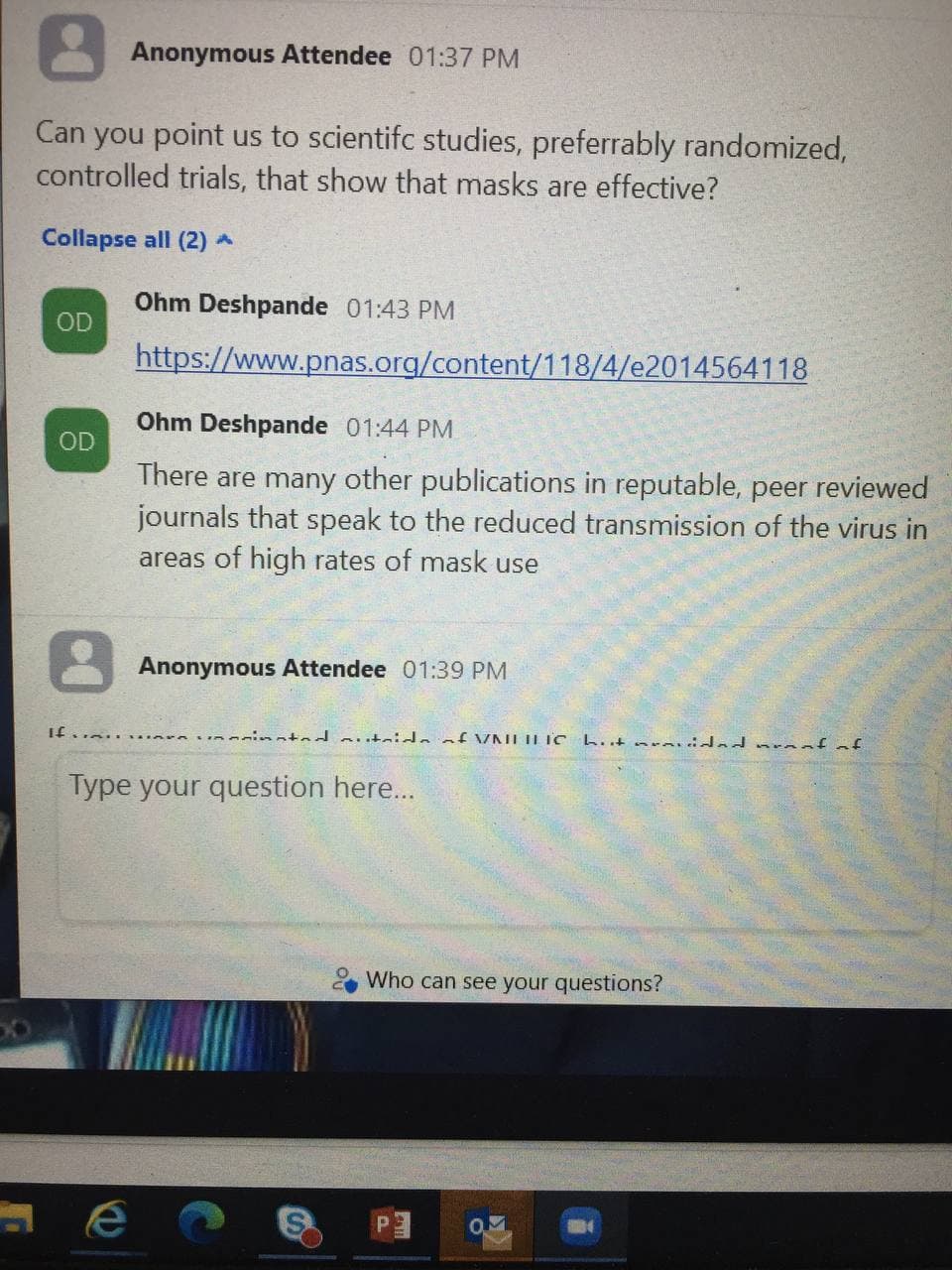
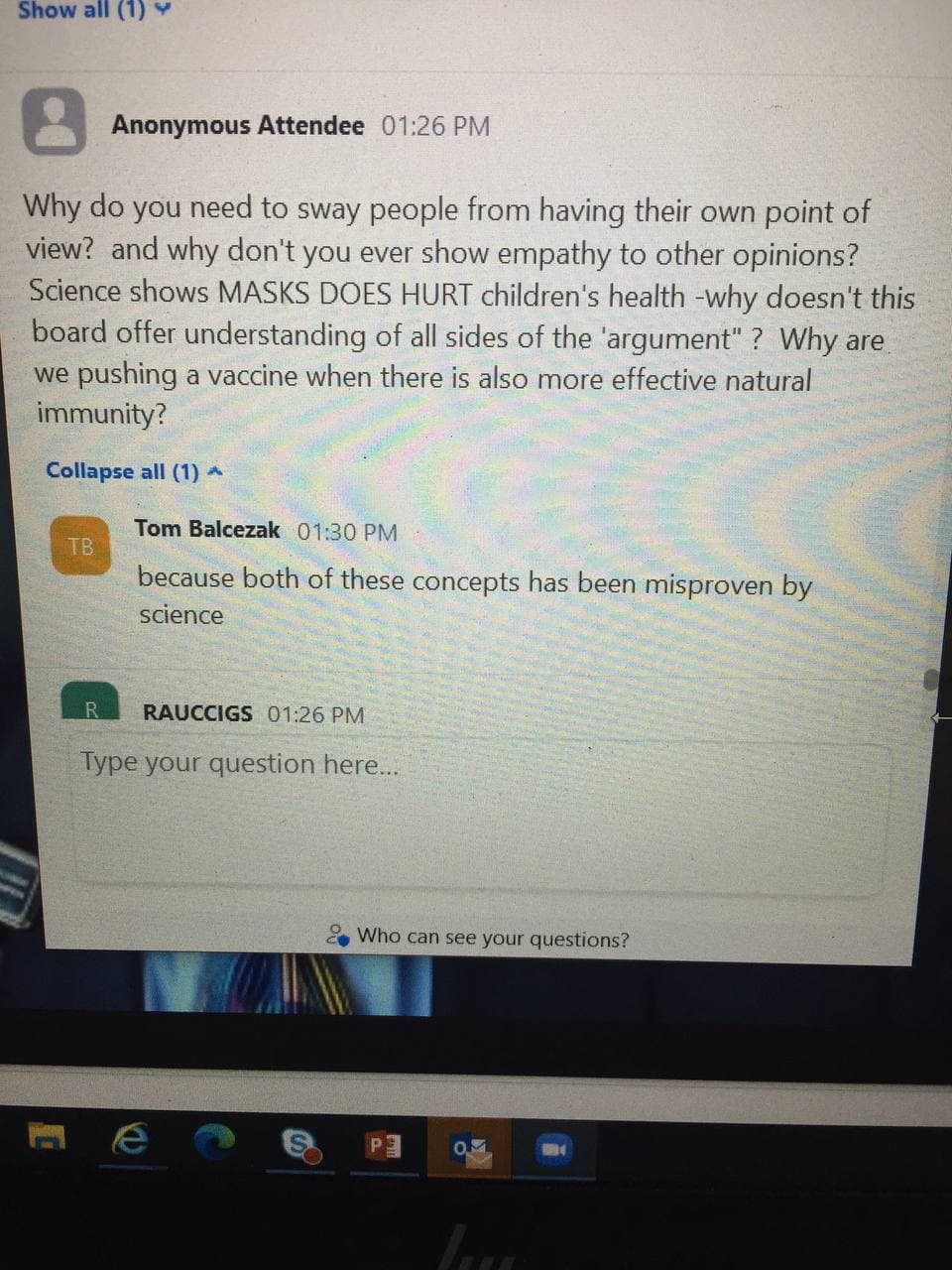
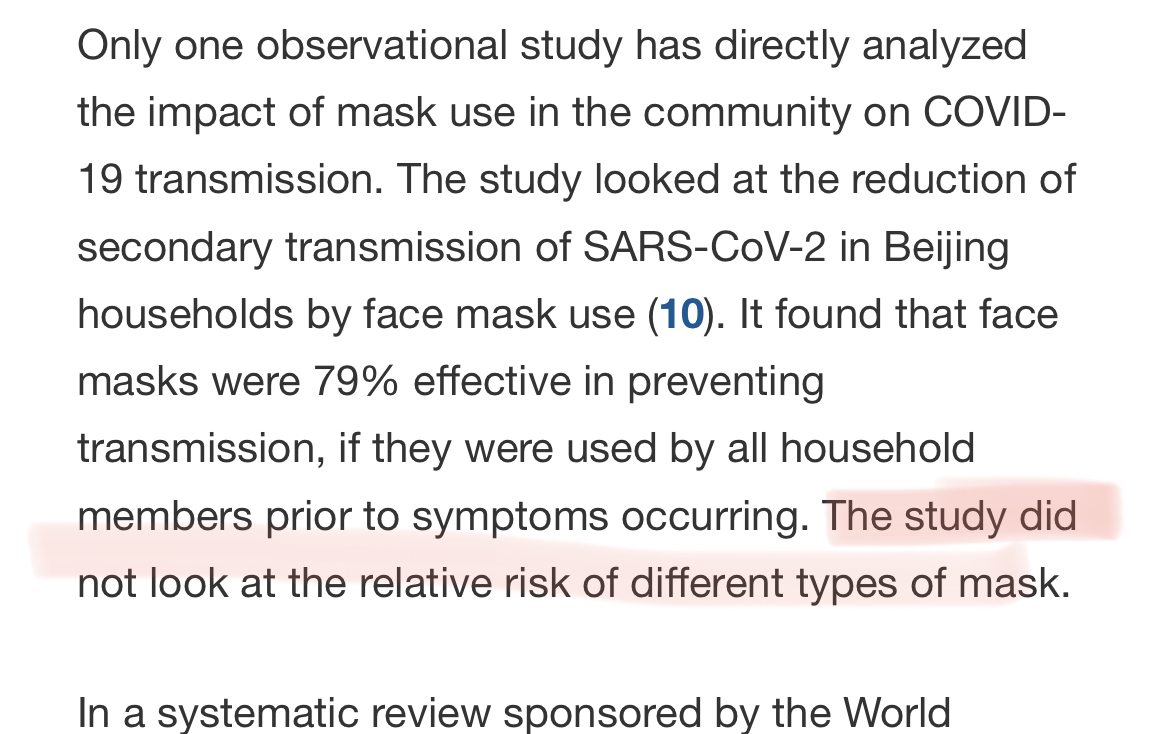
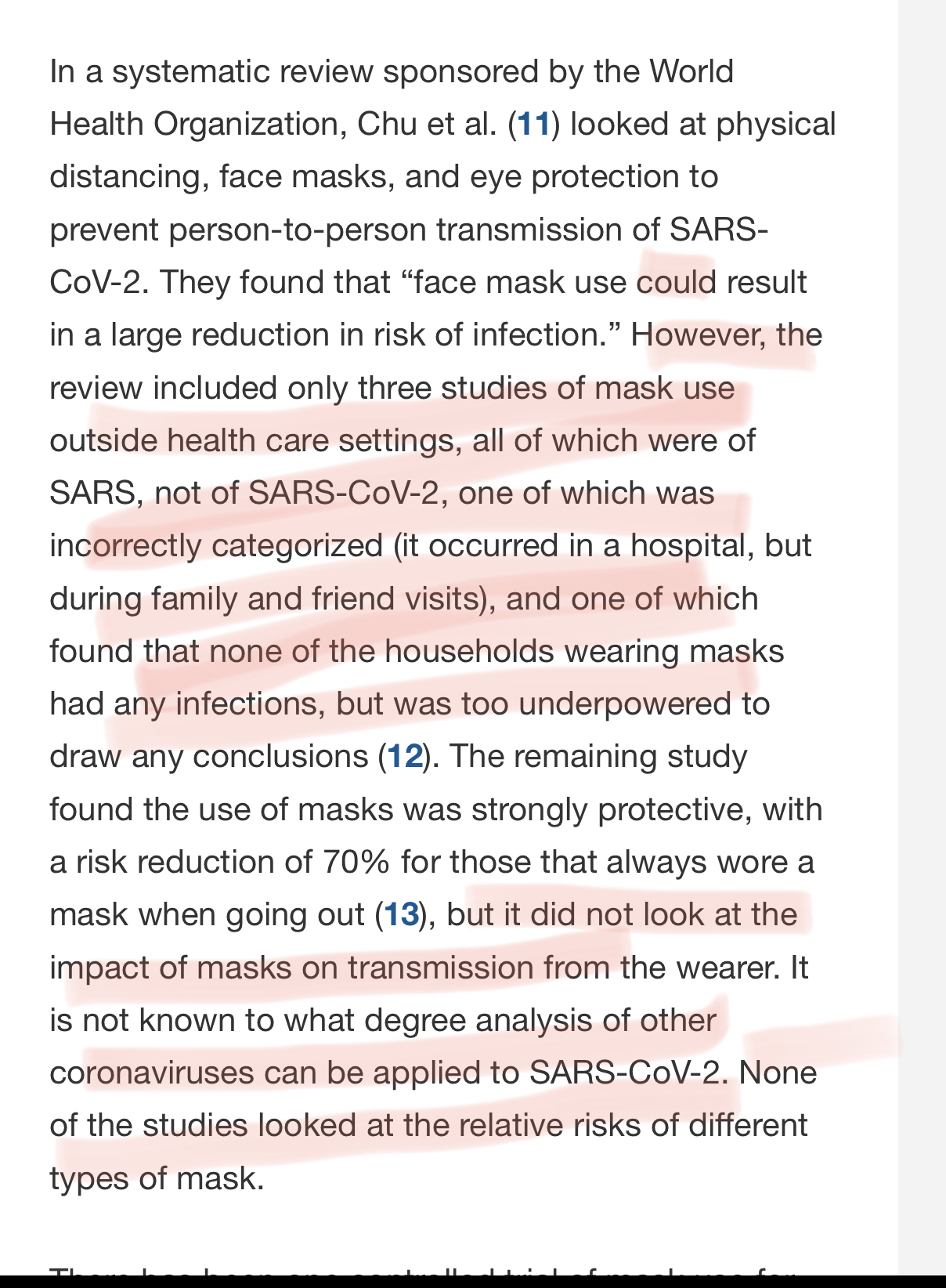
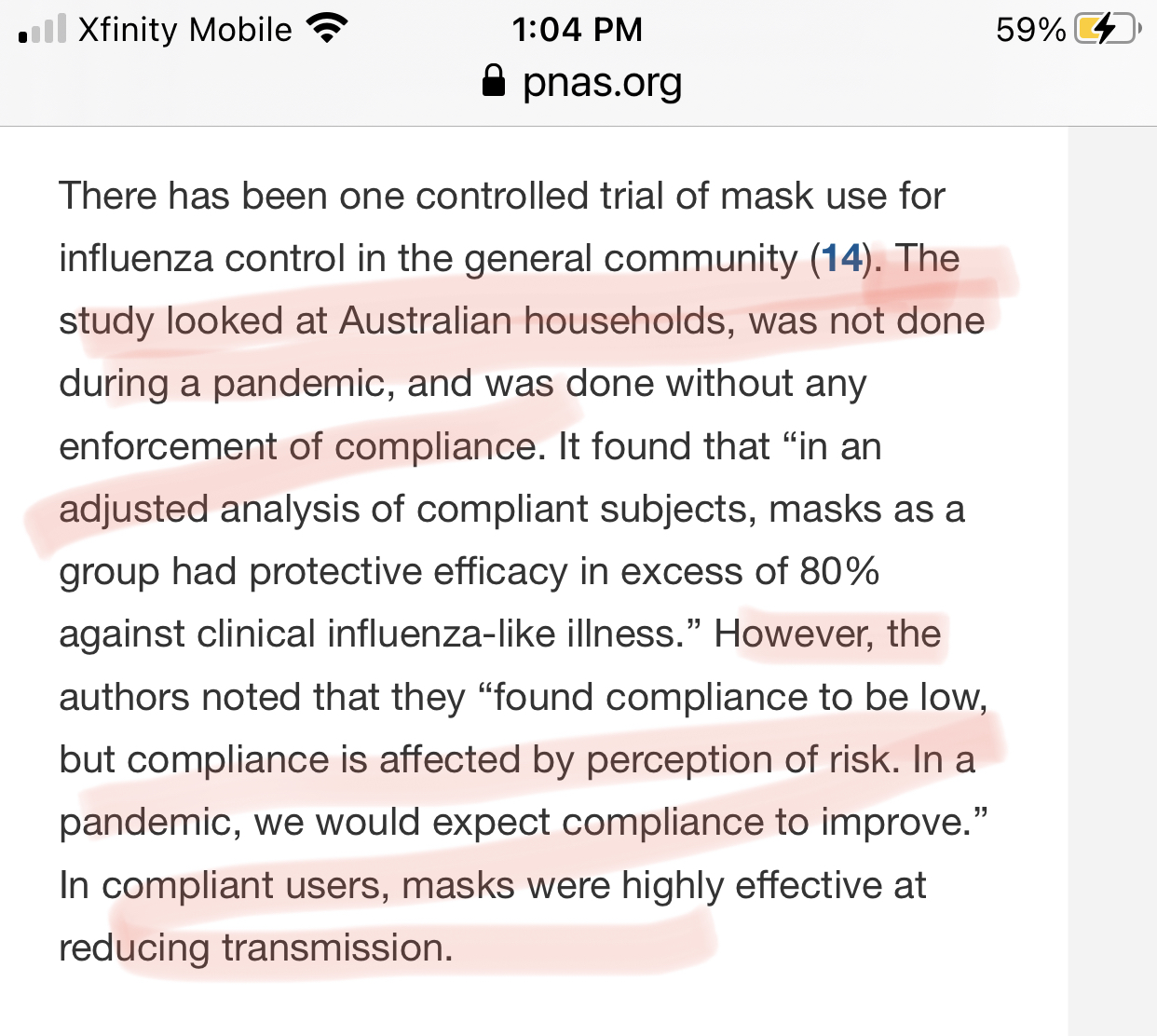
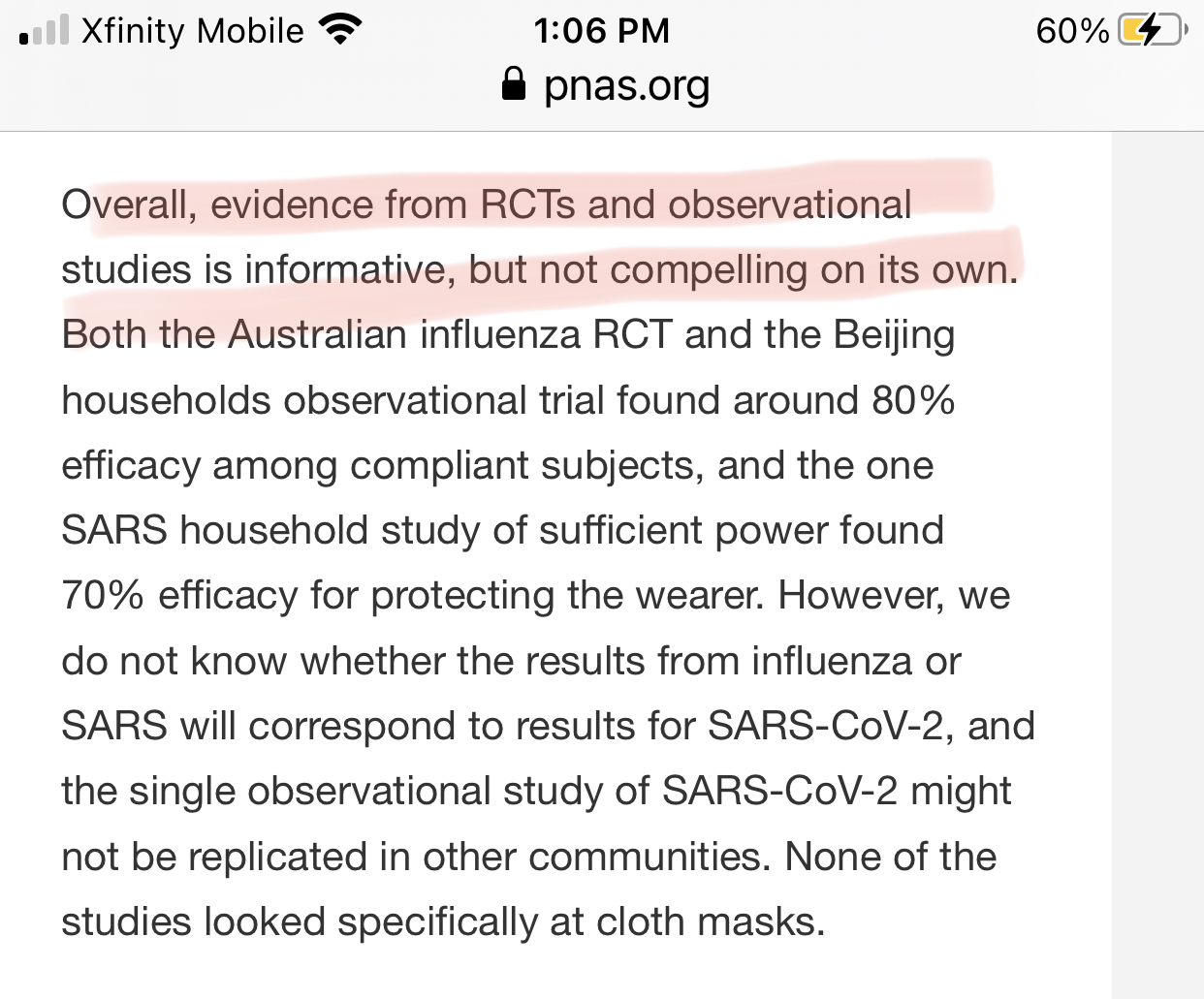
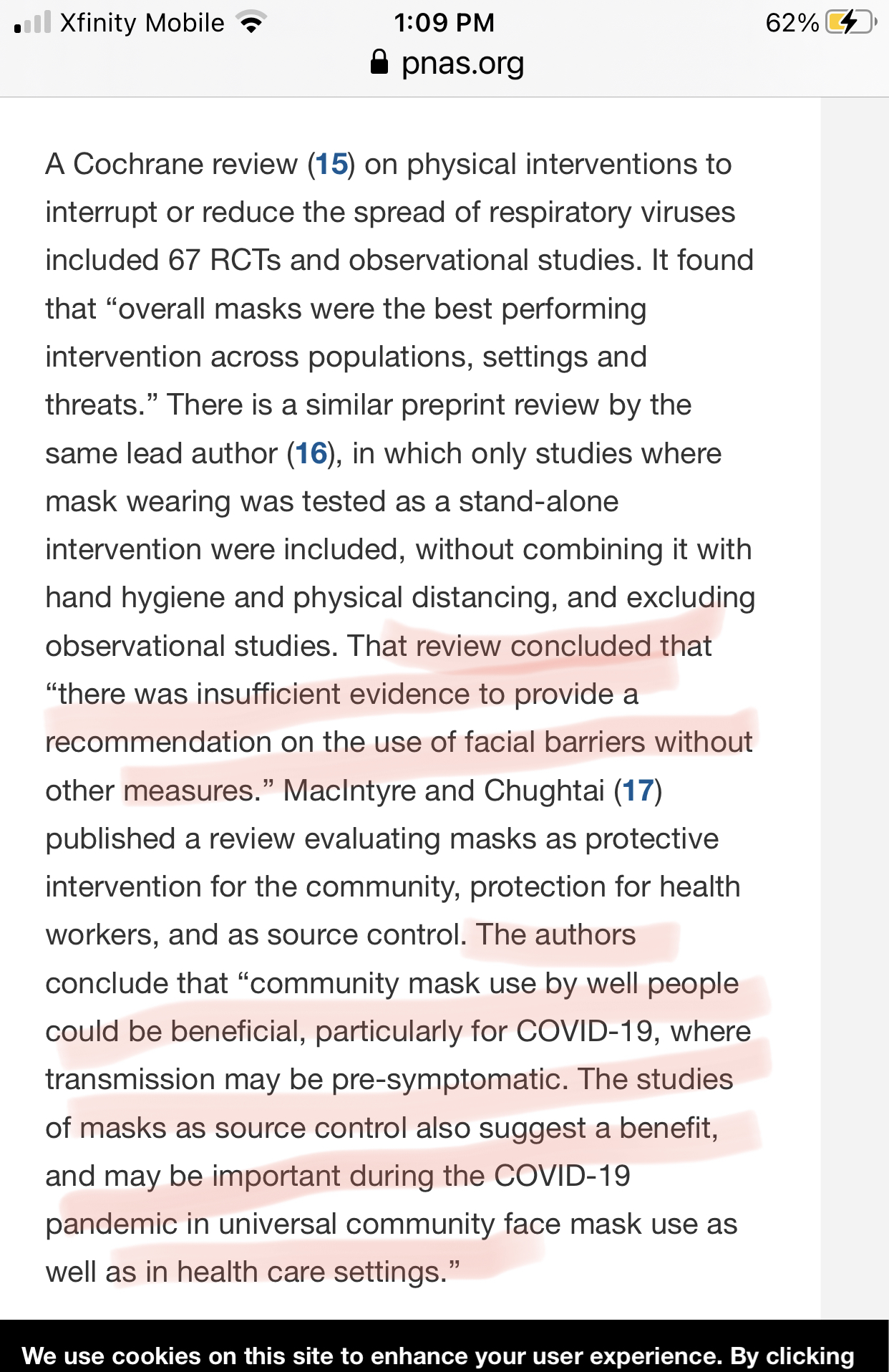
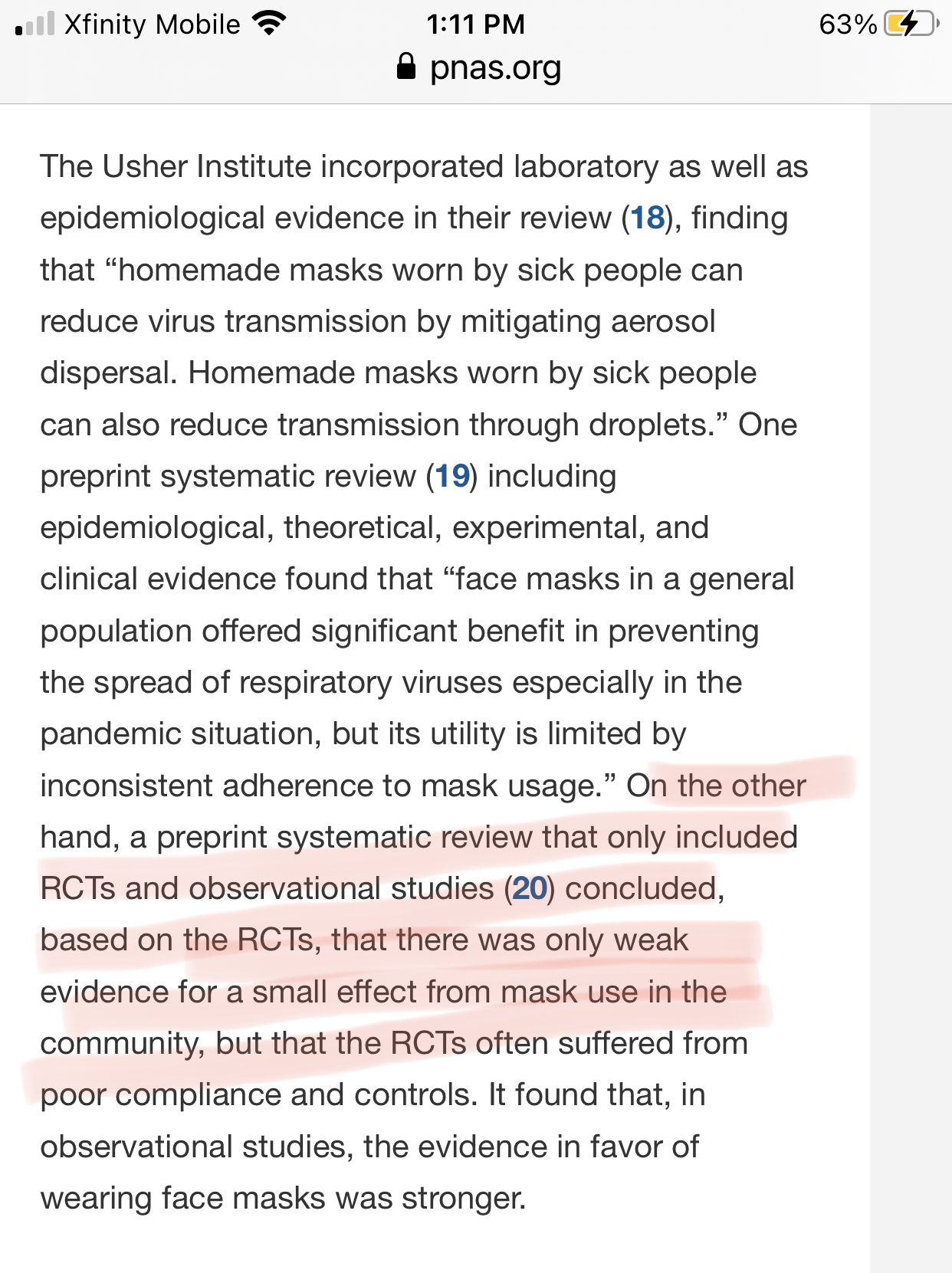
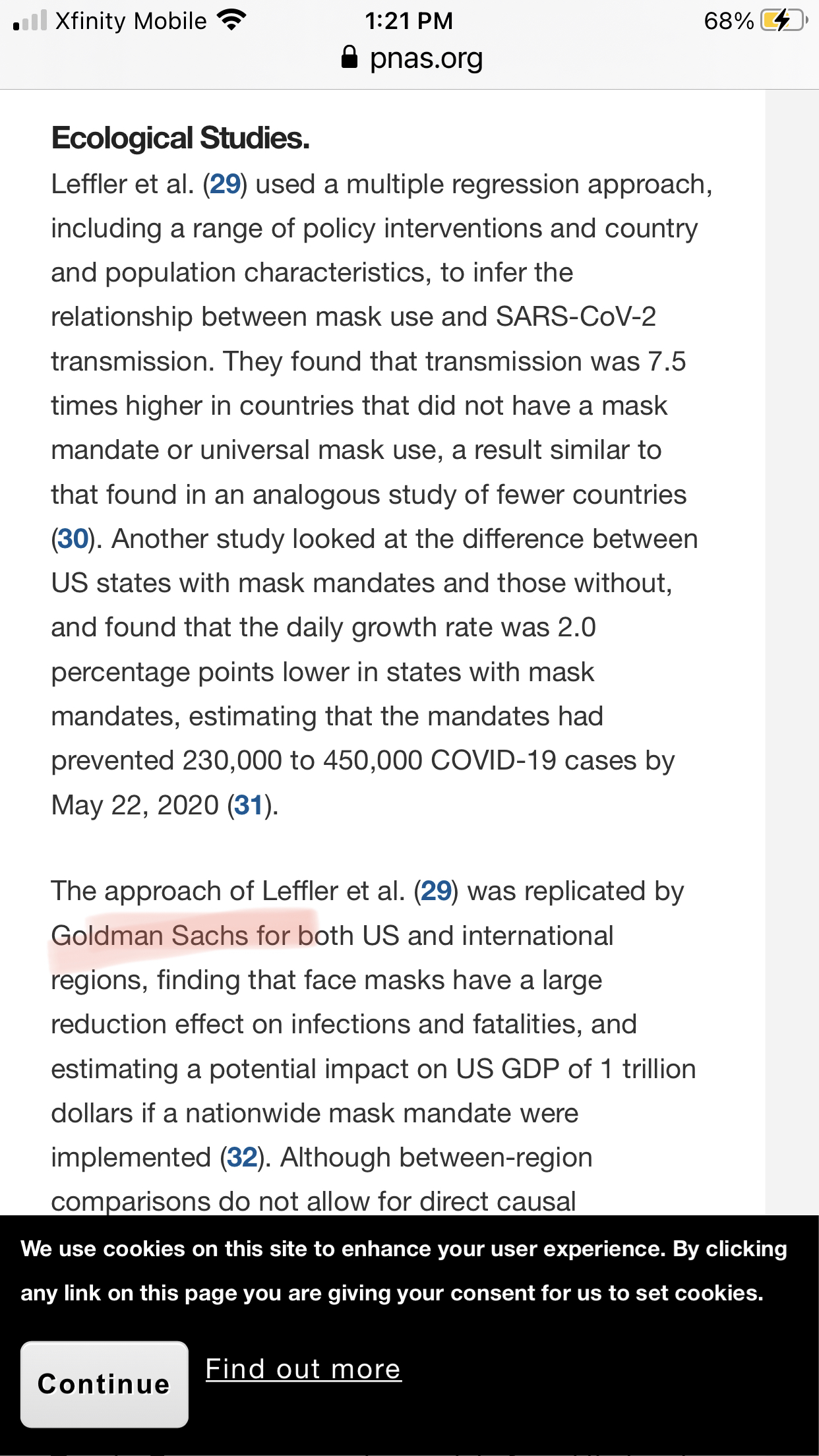
Yale on masks and patients concerns:
Here are snapshots of the study Yale New Haven is referring to. You can find the link to the full study in my resources. Things to note, this was a “narrative study” and Goldman Sachs did a study featured in this study. A new word in the medical field was found in the study, “pauci-symptomatic”, and it’s not a valid Scrabble word, just saying.
Yale New Have on Ivermectin.
Ivermectin Study from PubMed.gov
“Ivermectin, a US Food and Drug Administration-approved anti-parasitic agent, was found to inhibit severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) replication in vitro. A randomized, double-blind, placebo-controlled trial was conducted to determine the rapidity of viral clearance and safety of ivermectin among adult SARS-CoV-2 patients. The trial included 72 hospitalized patients in Dhaka, Bangladesh, who were assigned to one of three groups: oral ivermectin alone (12 mg once daily for 5 days), oral ivermectin in combination with doxycycline (12 mg ivermectin single dose and 200 mg doxycycline on day 1, followed by 100 mg every 12 h for the next 4 days), and a placebo control group. Clinical symptoms of fever, cough, and sore throat were comparable among the three groups. Virological clearance was earlier in the 5-day ivermectin treatment arm when compared to the placebo group (9.7 days vs 12.7 days; p = 0.02), but this was not the case for the ivermectin + doxycycline arm (11.5 days; p = 0.27). There were no severe adverse drug events recorded in the study. A 5-day course of ivermectin was found to be safe and effective in treating adult patients with mild COVID-19. Larger trials will be needed to confirm these preliminary findings.”
Ivermectin Study, The National Center for Biotechnology Information advances science and health by providing access to biomedical and genomic information.
Ivermectin for Prevention and Treatment of COVID-19 Infection: A Systematic Review, Meta-analysis, and Trial Sequential Analysis to Inform Clinical Guidelines
“Moderate-certainty evidence finds that large reductions in COVID-19 deaths are possible using ivermectin. Using ivermectin early in the clinical course may reduce numbers progressing to severe disease. The apparent safety and low cost suggest that ivermectin is likely to have a significant impact on the SARS-CoV-2 pandemic globally.“
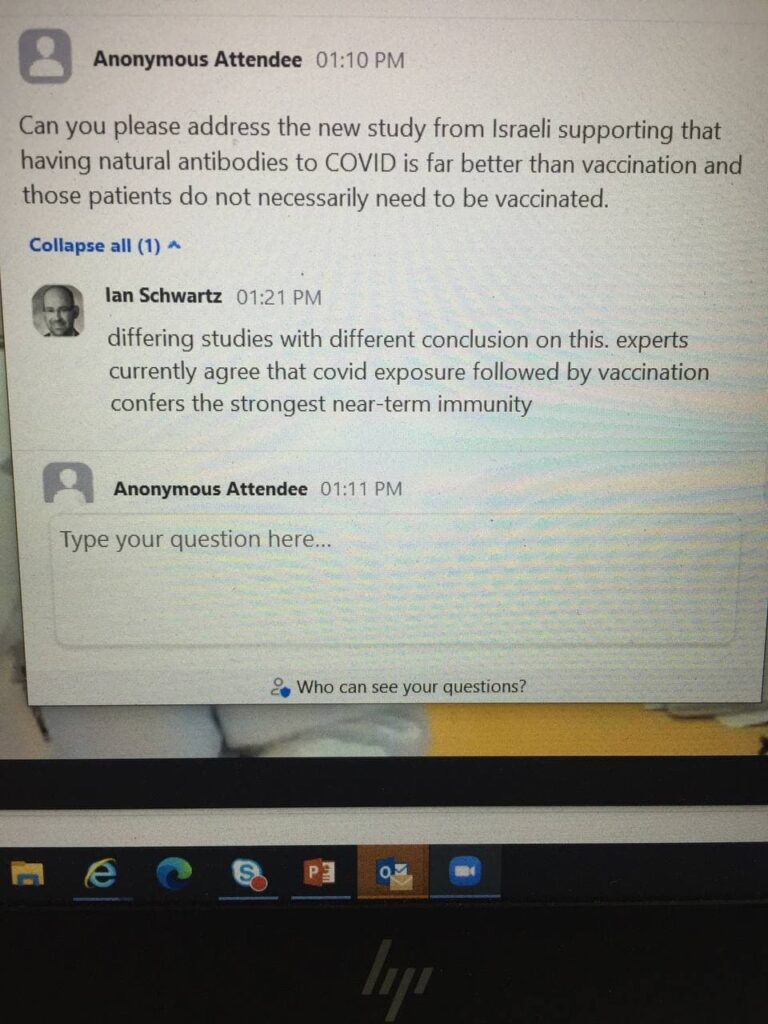
“The natural immune protection that develops after a SARS-CoV-2 infection offers considerably more of a shield against the Delta variant of the pandemic coronavirus than two doses of the Pfizer-BioNTech vaccine, according to a large Israeli study that some scientists wish came with a “Don’t try this at home” label. The newly released data show people who once had a SARS-CoV-2 infection were much less likely than never-infected, vaccinated people to get Delta, develop symptoms from it, or become hospitalized with serious COVID-19.”
Resources:
Assembly Bill A416 2021-2022 Legislative Session
VAERS
https://vaers.hhs.gov/about.html
HRSA
https://www.hrsa.gov/sites/default/files/hrsa/vaccine-compensation/data/data-statistics-report.pdf
VAERS Study
OpenVAERS.com
https://www.openvaers.com/covid-data/mortality
Comirnaty
https://www.fda.gov/media/151707/download
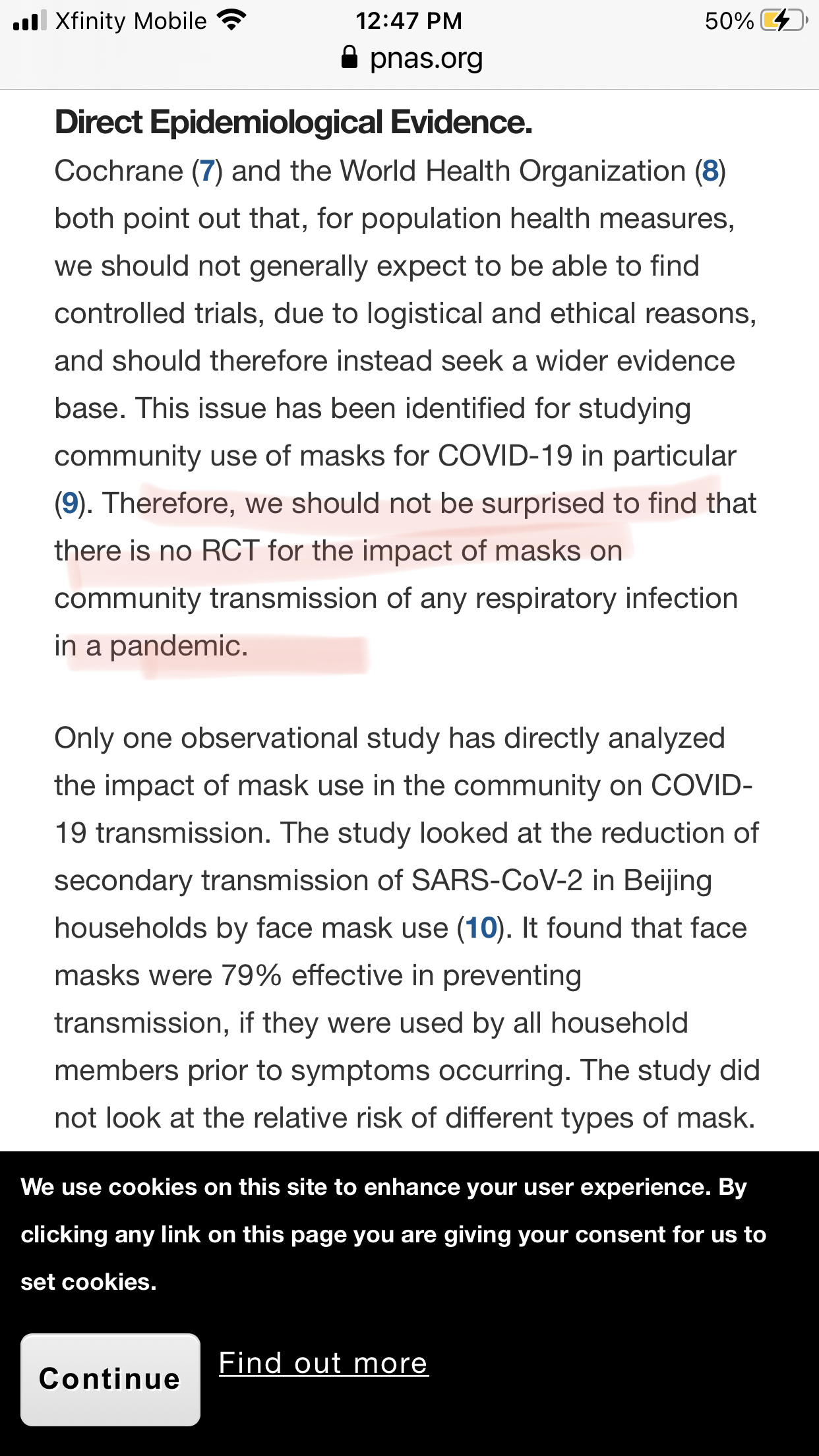
Mask Study
https://www.pnas.org/content/118/4/e2014564118
Israeli Study
Ivermectin
https://pubmed.ncbi.nlm.nih.gov/33278625/
The National Center for Biotechnology Information advances science and health by providing access to biomedical and genomic information.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8248252/
Informed consent disclosure to vaccine trial subjects of risk of COVID-19 vaccines worsening clinical disease
https://pubmed.ncbi.nlm.nih.gov/33113270/